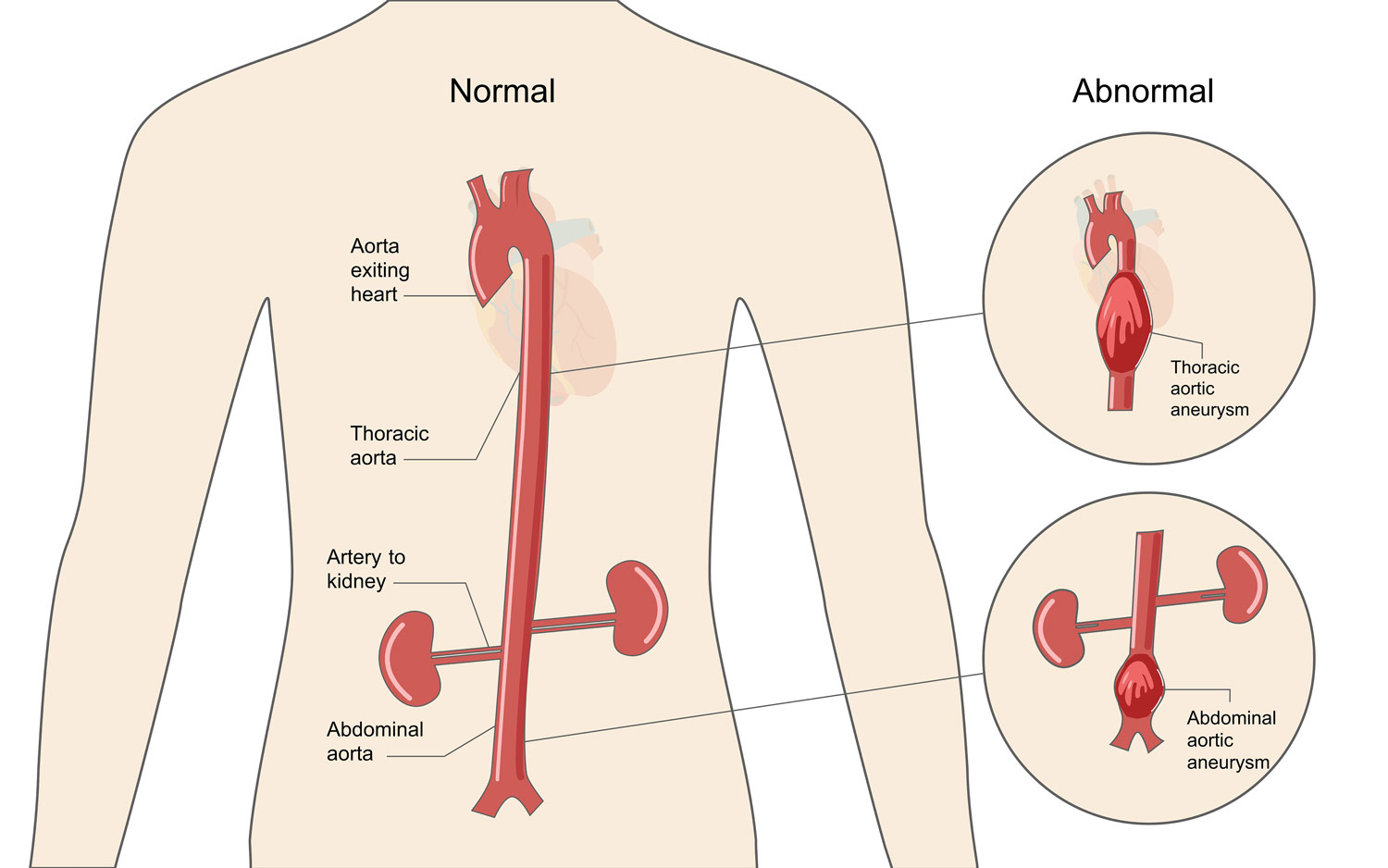
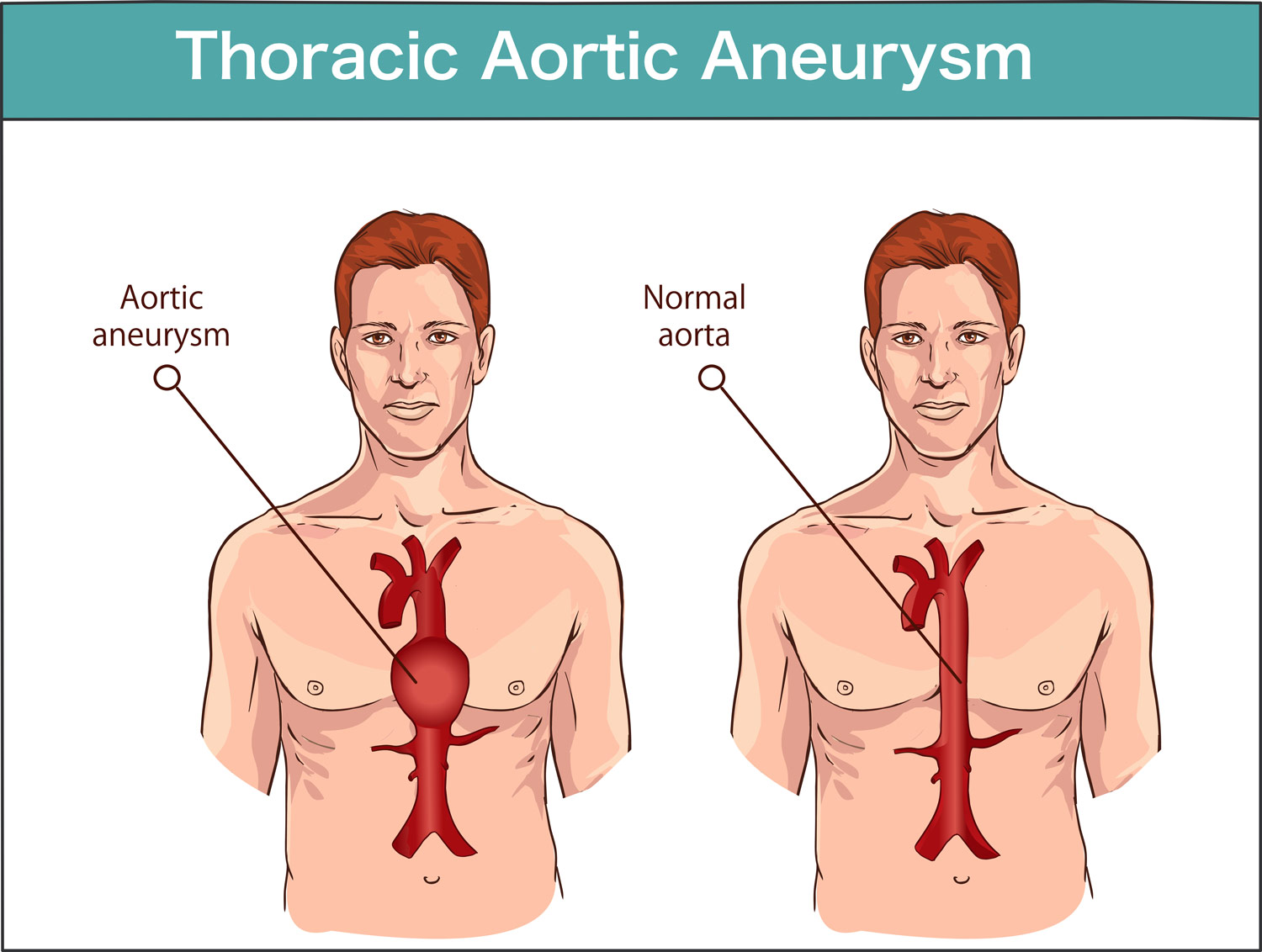
A thoracic aortic aneurysm is an enlargement of the aorta (the main blood vessel that carries blood away from the heart to the rest of the body) in the thoracic cavity or the chest area. This condition is fairly common in the general population, but about 20 percent of the cases are caused by a genetic condition.
Early detection, frequent imaging, and treatment are critical because both aortic aneurysms and dissections increase the risk that the aorta will suddenly burst (rupture), causing massive internal bleeding. Without surgery to prevent aortic rupture, these blood vessel abnormalities can be life-threatening.
What are the Key Features of Familial Thoracic Aortic Aneurysm and Dissection?
Aortic enlargement (dilatation/aneurysm) is generally the main feature of this condition. Aortic dissection is a sudden tear of the inner wall of the aorta that allows blood to flow between the aorta’s inner and outer walls. This causes chest and/or back pain and can lead to aortic rupture. People may develop aneurysms or aortic dissections at any time in their lives. This condition can be inherited and, even within the same family, the occurrence and timing of these problems can vary.
When a person or family members have these features, it is important for the extended family to be evaluated by a cardiologist and geneticist.
You may contact our Help & Resource Center with questions anytime at marfan.org/ask or download our fact sheet.
What are the Causes of Familial Thoracic Aortic Aneurysm and Dissection?
About 20 percent of people with thoracic aortic aneurysm and dissection have a genetic predisposition to it, meaning it runs in the family. This type is known as familial thoracic aneurysm and dissection. Many people don’t know they have a genetic predisposition to thoracic aortic aneurysm and dissection. First-degree relatives (i.e., parents, children, siblings) of individuals known to have thoracic aortic aneurysm should be screened for the condition.

Getting Diagnosed with Familial Thoracic Aortic Aneurysm and Dissection
Thoracic aortic aneurysm and dissection is diagnosed based on the presence of dilatation and/or dissection of the thoracic aorta and the absence of clinical features of other connective tissue disorders, such as Marfan syndrome, Loeys-Dietz syndrome, or vascular Ehlers-Danlos syndrome. Speak to your doctor about differential diagnosis for these connective tissue disorders and possibly getting a genetic test (aortic panel) that screens for multiple genes.
A diagnosis of familial thoracic aortic aneurysm and dissection is made when there is a positive family history of aneurysm and dissection.
Aortic aneurysms are diagnosed using imaging techniques such as echocardiography (sound wave picture), computed tomography (CT or CAT scan), magnetic resonance imaging (MRI), transesophageal echocardiogram (TEE), chest x-ray, or angiography. Aortic dissections can be diagnosed through computed tomography (CT or CAT scan) or transesophageal echocardiogram (TEE). There are many known genes to cause FTAAD but there are still many genes that need to be discovered.
How is Familial Thoracic Aortic Aneurysm and Dissection Managed?
The management of familial thoracic aortic aneurysm and/or dissection requires the coordinated input from a multidisciplinary team of specialists familiar with this condition, including a medical geneticist, cardiologist, and cardiovascular surgeon.
Medications (drugs) that reduce the stress on the aorta can be helpful. Beta-blockers help lower blood pressure and reduce the force of the heartbeat. They also may help prevent or slow aortic enlargement and reduce the risk of aortic dissection.
People with familial thoracic aortic aneurysm and dissection must have routine tests to monitor their aortic health and identify problems before there is an emergency. These are the same imaging tests that doctors use to diagnose the condition: echocardiogram, MRI, CT scan, or TEE.
For individuals with an ACTA2 mutation, screening for coronary artery disease and cerebrovascular disease is reasonable. For individuals with a TGFBR1, TGFBR2, TGFB2, or SMAD3 mutation, annual imaging of the aorta and its branches and cerebrovascular circulation is recommended.
Surgery is most effective if it is done before an aortic dissection or other life-threatening situation. Surgery is considered when:
- The rate of enlargement of the ascending aorta approaches 0.5 cm per year
- The diameter of the ascending aorta is between 4.2 and 5.0 cm (depending on the underlying mutation or family history)
The two most common types of surgery are:
- The Bentall procedure, which involves an aortic graft repair plus insertion of an aortic mechanical valve. After this surgery, a patient is required to take blood-thinning medication for the rest of their life to avoid blood clots, which could be life-threatening.
- Valve-sparing surgery, which replaces the damaged part of the aorta, but keeps the patient’s own aortic valve. This type of surgery, which does not require blood-thinning medication afterward, can only be performed if the patient’s valve is working properly.
Regardless of which type of surgery is performed, patients must continue to take their blood pressure medicine and have their aorta monitored at least once a year to safeguard against additional enlargements or tears in other parts of the aorta.

Have a question?
We can help.
Contact our Help & Resource Center by submitting a question via the link below.
Emergency Preparedness
Following your doctor’s recommendations for medication, monitoring, and physical activity gives you the best chance of avoiding a serious complication of familial thoracic aortic aneurysm and dissection. Still, there are no guarantees. That’s why it’s important for you to learn about the medical problems that could arise and require immediate medical treatment.
To help prepare you for these situations, we recommend that you complete our Emergency Preparedness Kit, which we created specifically for people with Marfan syndrome and related conditions. It includes our Emergency Alert Card which you can download and carry in your wallet. You can click below to download them.